Newer modalities for treatment of Meibomian Gland Dysfunction and Evaporative dry eye
With an improved understanding of the pathophysiology and manifestations of dry eye, a plethora of new diagnostic and treatment modalities have become available, particularly in the treatment of Meibomian gland dysfunction (MGD) associated evaporative dry eye. This section will discuss some treatment modalities which have brought about a qualitative change in the approach.
Limitations of conventional warm compresses and manual lid expression
Warm compresses with manual lid expression continues to be the first line of treatment for Meibomian Gland Dysfunction. However, the glands are situated towards the inner surface of the eyelids and require a temperature of 32 – 45 O Celsius1 to melt meibum, thereby consistenly requiring more than 45 O Celsius on the external surface of the eyelids. Retaining this heat with a facecloth is often not possible.
Additionally, it has been found that the pressure for the evacuation of expressible contents from the Meibomian glands ranges from 10 – 40 psi. Only 7 % patients are able to tolerate this degree of pressure.2
Due to the above reasons, compliance is a challenge, and even in the compliant individuals, the desired results are often not attained
Lipiflow
Lipiflow, or Vector Thermal Pulsation (Johnson & Johnson Vision, USA) overcomes these limitations by providing controlled outer directional heat and intermittent pressure to the eyelids, to facilitate release of lipids from the meibomian glands.

Figure 1 : Lipiflow Vector thermal pulsation system with eyepiece activator
The lipiflow system does this using a sterile disposable eyepiece activator connected to the console. The activator itself comprises of 2 parts:
- Lid warmer – Composed of a heater, eye insulation and vaulted shield. This provides heat to the palpebral surface of the upper and lower eyelids directly at the level of the Meibomian glands
- Eye Cup – Composed of an inflatable air bladder and rigid activator. This delivers graded pulsatile pressure to the outer eyelid
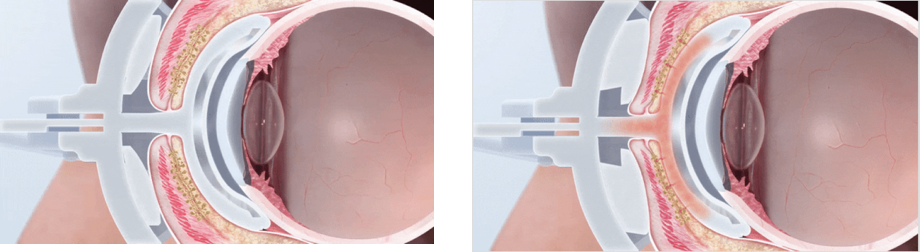
Figure 2 : Application of heat and pressure during treatment with lipiflow
Various studies have looked at the clinical efficacy of Lipiflow and have found improvement in dry eye parameters such as Tear Breakup Time (TBUT), Lipid Layer Thickness (LLT), and reduction in OSDI and SPEED scores indicating symptomatic improvement. The duration of effect has been found to be between 6 months and 2 years.
Limitations
- The procedure is extremely expensive and most patients are unable to afford it.
- Individuals with extensive Meibomian gland dropouts (as seen on meibography) are usually refractory to any treatment and such patients may instead be managed by conventional measures with explanation of poor prognosis.
Mibo Thermoflo
The Mibo Thermoflo (Mibo Medical, USA) is a therapeutic device which supplies continuous heat to the external surface of the eyelids. The eyelids are gently massaged with the probe using an ultrasound gel which helps liquefy the contents of the Meibomian glands, following which they can be manually expressed.

Figure 3 : Mibo Thermoflo
Limitations
- Heat is applied from the external surface
- No pressure pulsations are applied in the treatment. The glands need to be manually expressed after treatment
Eyelid Heating masks
Various heating masks such as MGDRx Eyebag (®), EyeDoctor (®), Bruder (®), Tranquileyes XR™, Thera°Pearl (®) are now available. Comparative studies have shown stable heat retention throughout the treatment cycle, and have found all of these to be better than conventional warm compresses with facecloth.3
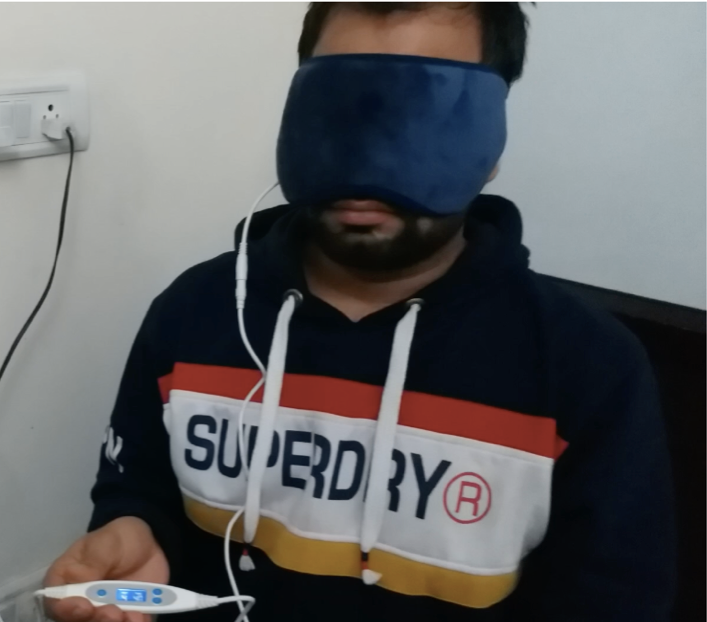
Figure 4 : USB-based heating mask
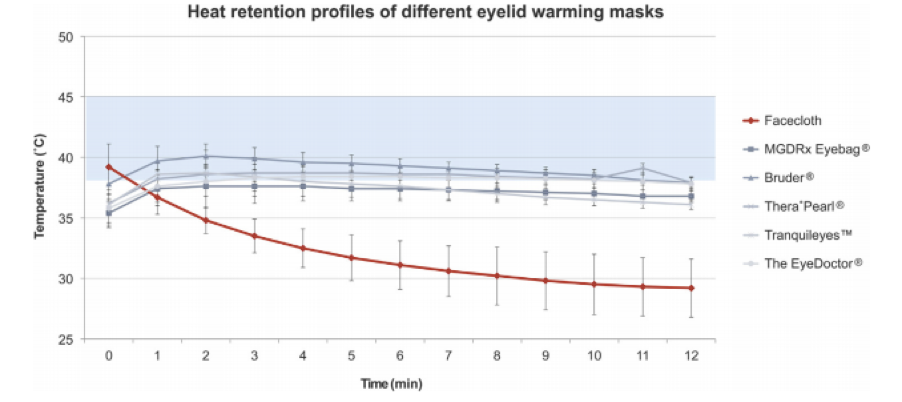
Figure 5 : Heat retention profiles of eyelid masks versus Facecloth (Source :E. Bitton et al. / Contact Lens & Anterior Eye 2015)
The modalities discussed above have also been compared in terms of heat achieved at the inner surface of eyelids, of which Lipiflow was found to be the most effective in attaining the surface temperatures of 40O. 4
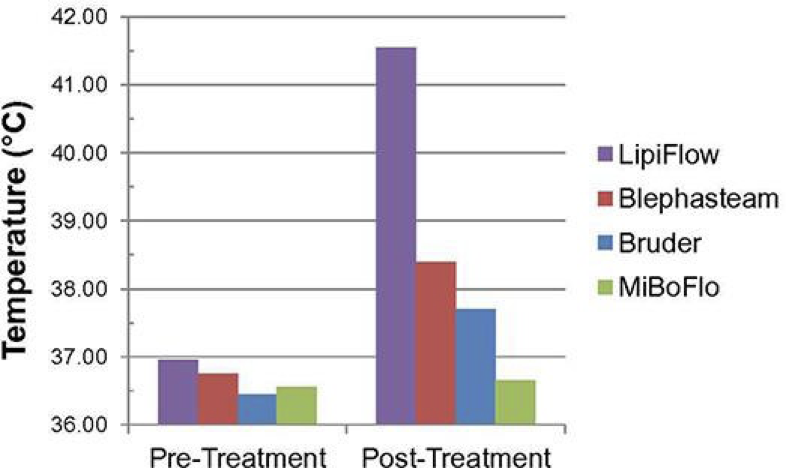
Figure 6 : Temperatures at the inner surface of eyelids (Source : Kenrick CJ et al, Case Rep Ophthalmol 2017)
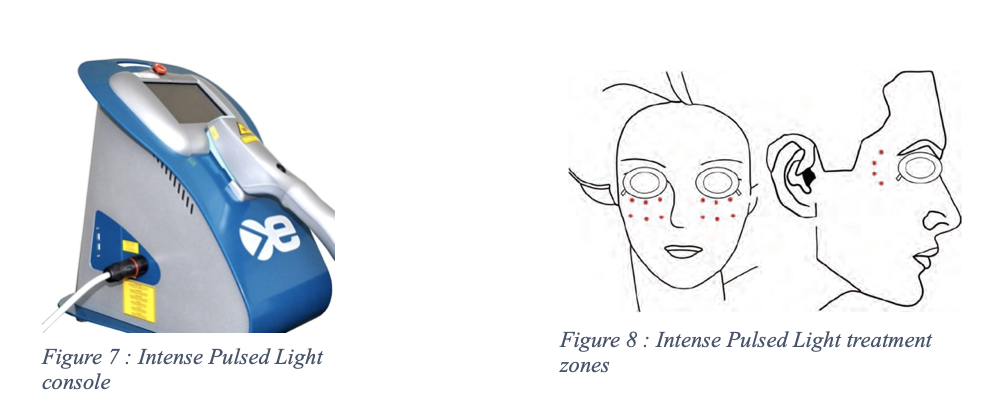
Intense Pulsed Light (IPL)
Intense Pulsed Light, previously used extensively for Rosacea and other skin conditions is now gaining popularity in the treatment of Meibomian Gland Dysfunction. IPL is a polychromatic light source with a wavelength spectrum of 500 – 1200 nm, which can be filtered to allow only a range of wavelengths to be emitted5. The procedure involves placement of the probe along with ultrasound gel on 10 -15 spots on either side of the face during the treatment cycle. Application is repeated for a total of two passes on each side.
The mechanism involves selective thrombosis of the vessels surrounding the Meibomian glands which leads to regression of telangiectatic vessels and reduction of the access of inflammatory mediators. In addition to this, the heat generated helps liquefy the contents of the glands.
Limitations
- Treatment is limited to Fitzpatrick skin type IV or lighter, as there is a greater risk of skin pigmentary changes in darker individuals
- Though the treatment is relatively safe, some ocular complications including uveitis, iris atrophy and pupillary defects6 have been documented . A case of corneal pigment deposition after IPL treatment in an individual wearing coloured contact lenses has also been reported.
iLux
The iLux MGD Treatment System (Alcon, USA) is a handheld device that provides light-based heat and compresses the meibomian glands to express them. The sterile tip comprises an inner pad which slips behind the eyelid and the outer pad which compresses it using a single-click button. Temperature sensors measure the inner and outer lid temperature to maintain a meibum melt temperature of 38-42 O Celsius.

Figure 9 : iLUX device (Image Source : Tauber et al. Clinical Ophthalmology 2020)
A recent study comparing the iLux device and Lipiflow has found that both are comparable in terms of safety and efficacy, with no clinically meaningful or statistically significant differences between the two.8
Limitation
A more recent device, there is limited literature on efficacy and safety. More controlled studies targeted on our population will help establish its role more clearly
Summary
With a wide range of devices now available to treat Meibomian gland dysfunction and associated evaporative dry eye, the clinicians are flooded with options. It is important for each practitioner to take individual decisions on which modality/modalities are the most suitable in their practice, keeping in mind the nature of practice, the prevalence of dry eyes and the affordability of their patients. In a value-centric country like India, the perceived benefit from various treatments may vary depending on the affordability and that has to be kept in mind before choosing which modality to offer. Additionally, a trial of warm compresses and manual lid expression, though less effective provides a reasonable starting point and also justifies the need for additional treatment if the patient is not improving symptomatically.
Author
References
- Borchman, D. et al. Human Meibum Lipid Conformation and Thermodynamic Changes with Meibomian-Gland Dysfunction. Investig. Opthalmology Vis. Sci. 52, 3805 (2011).
- Korb, D. R. & Blackie, C. A. Meibomian Gland Therapeutic Expression: Quantifying the Applied Pressure and the Limitation of Resulting Pain: Eye Contact Lens Sci. Clin. Pract. 37, 298–301 (2011).
- Bitton, E., Lacroix, Z. & Léger, S. In-vivo heat retention comparison of eyelid warming masks. Contact Lens Anterior Eye J. Br. Contact Lens Assoc. 39, 311–315 (2016).
- Kenrick, C. J. & Alloo, S. S. The Limitation of Applying Heat to the External Lid Surface: A Case of Recalcitrant Meibomian Gland Dysfunction. Case Rep. Ophthalmol. 8, 7–12 (2017).
- Vora, G. K. & Gupta, P. K. Intense pulsed light therapy for the treatment of evaporative dry eye disease: Curr. Opin. Ophthalmol. 26, 314–318 (2015).
- Lee, W. W., Murdock, J., Albini, T. A., OʼBrien, T. P. & Levine, M. L. Ocular Damage Secondary to Intense Pulse Light Therapy to the Face: Ophthal. Plast. Reconstr. Surg. 27, 263–265 (2011).
- Hong, S., Lee, J. R. & Lim, T. Pigment Deposition of Cosmetic Contact Lenses on the Cornea after Intense Pulsed-Light Treatment. Korean J. Ophthalmol. 24, 367 (2010).
- Tauber, J., Owen, J., Bloomenstein, M., Hovanesian, J. & Bullimore, M. A. Comparison of the iLUX and the LipiFlow for the Treatment of Meibomian Gland Dysfunction and Symptoms: A Randomized Clinical Trial. Clin. Ophthalmol. Volume 14, 405–418 (2020).