 Introduction:
Introduction:
The ophthalmic imaging has now revolutionized with the deployment of smartphone for the image acquisition. The widespread adaptability is due to multiple factors, the forefront of which are the availability of good resolution cameras in mid and high-end smartphones, good auto-focusing mechanism, in-built high capacity storage, internet capabilities that enable cloud storage and teleconsultation capabilities, and the option to use specifically developed application or artificial intelligence solutions due to the high processing power of these modern-day smartphones. The testament to the success of these smartphone-based devices is the entry of multi-national giants like Keeler and Volk in this segment to compete with the homegrown companies like MII RetCam Inc and Remidio.[1–4] The germinal idea of smartphone imaging is so minimalistic that you will often see articles with DIY projects to make anterior segment imaging modules and fundus cameras.[5,6]
While the anterior segment and fundus smartphone-based or smartphone assisted imaging techniques were percolating the ophthalmology community, the imaging of anterior chamber angle anatomy never caught the fancy. The less than warming response of the innovators stem from the fact that gonioscopy is somehow considered a difficult skill to master, a fact that is not helped by the time it takes to perform a complete gonioscopy examination with a 3 mirror goniolens, one of the most common lenses used for the OPD based evaluation. The ophthalmologists get used to the surrogate of gonioscopic anatomy i.e. the von-Herrick grading of anterior chamber depth. A survey has revealed about half of the patients visiting a “Glaucoma Clinic” do not get a gonioscopic evaluation done before treatment.[7] The Asian population has a considerably higher proportion of angle-closure glaucoma. A population-based survey in India has demonstrated an almost equal distribution of open and closed-angle glaucoma.[8] To extrapolate, the magnitude of angle-closure suspects will still be higher but are missed in the routine evaluation due to the gonioscopy not being practiced routinely.
The smartphone-based gonio-imaging, like the traditional gonioscopy, somehow was dependent on the slit-lamp before we published a novel slit-lamp independent gonio-imaging technique.[9,10] The slit-lamp imaging applies the same principle of placing the smartphone camera centered on one of the eye-piece to image anything that can be viewed on slit-lamp. A more systematic approach is to use a beam splitter to send a part of the incoming rays from the patient’s eye to the smartphone sensor so that the binocularity of the slit-lamp is maintained along with a permanently placed imaging accessory. While this technique helps you to image the anterior segment, gonioscopic anatomy, or the fundus seen through the slit-lamp, it is limited by its dependence on a slit-lamp. To be used freely in any setting such as clinical, optometry room, mobile eye clinics, or outreach camps, the imaging devices need to break the shackles of the slit lamp and become truly portable.
The Need of Society:
Glaucoma has been unfortunately but aptly titled as “the silent killer of vision” due to its slow contraction of visual fields until only tubular vision remains. WHO defines “Glaucoma can be regarded as a group of diseases that have as a common end-point a characteristic optic neuropathy which is determined by both structural change and functional deficit.”[11] The prevalence of the disease is projected to affect 111.4 million by the year 2040. Currently, 4.5 million people worldwide have blindness attributable to primary glaucoma, accounting for 12% of the total blindness burden. India is estimated to account for 12.9% of Primary Open Angle Glaucoma (POAG) and 12.7% of Primary Angle Closure Glaucoma (PACG) global burden. Population-based surveys indicate PACG to be more attributing to the blindness than POAG.[12] The only method to diagnose the type of glaucoma is gonioscopy. But as iterated earlier, the gonioscopic evaluation is not as readily dispensed as it should be. The unmet need of gonioscopy we hypothesize can be eliminated by the introduction of a method that can be performed quickly in any setting (clinical or outreach camp) and provide reproducible results.
The Solution:
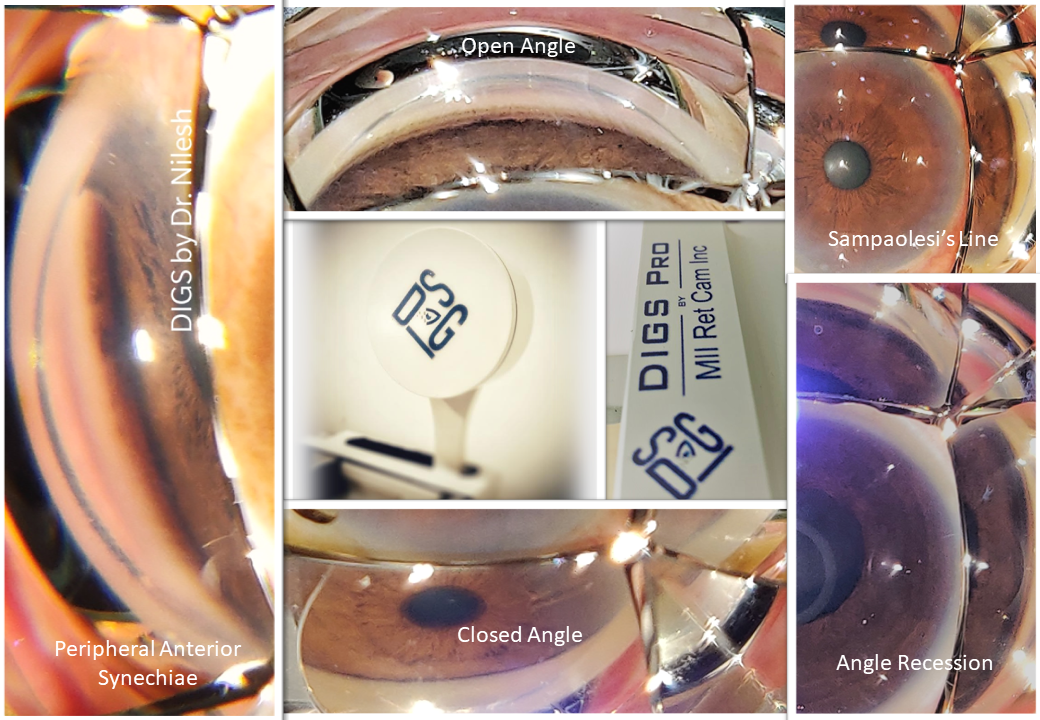
The need for the gonioscopy, coupled with dispensing the counseling to the patients with closed angles visiting the outreach camps to come to the base hospital for the laser iridotomy is a troubling thought. While tinkering on the idea, it was an accidental observation that the gonioanatomy is visible to the naked eye also when someone else was performing the gonioscopy. This got me into a zone of creative visualization about using a smartphone camera to image the angle and then using the image to classify the angle as well as to counsel the patient. The germinal idea of our slit-lamp independent smartphone-based gonio-imaging technique was subsequently published based on the imaging of 65 eyes which yielded an acquisition rate of clear images of 65% and the gradable quality images were 80% of the total. The technique was later christened as Direct Imaging of Goniomirror by Smartphone (DIGS). [https://youtu.be/j-J2oZCuBmA]
The DIGS though provided a simple and effective solution of the image the angle, which excited the ophthalmologists and was awarded at various platforms, the adoption by the community was underwhelming. The roadblock that we realized was twofold, first being the majority of physicians who have become comfortable performing the ocular examination without the gonioscopy included, and the other being that DIGS was a do-it-yourself (DIY) project which was thought to be time taking in a busy OPD.
The DIY project to a Product:
During discussions with my mentor Dr. Ashish Sharma, an accomplished innovator himself advised me to work on a product idea that will make DIGS a standardized and easy-to-use device. He told me to “convert my jugaad into a true innovation”, the words that became my guiding light through the journey. With the gracious help of his by providing me his team of designers and engineers who converted my rough sketches into prototypes which went through multiple stages of validation to finalize the optics, the distance, and the ergonomics to become the World’s First Smartphone-Based Gonio-Imaging Device -DIGS Pro, which is now into commercial production by MII RetCam Inc, Coimbatore and is a completely Make in India initiative. [https://youtu.be/PoV_UakpIwM] The product is now pending for patent, an important step that should be taken by all the innovators to protect their intellectual property.
DIGS Pro has been validated to be used with the 2-mirror, 3-mirror, 4-mirror, and 6-mirror goniolenses, all of which were compatible with DIGS. The 4-mirror and 6-mirror goniolenses are best suited for screening as they provide the gonioanatomy of all the quadrants in a single image thus making it a very rapid process. The validation study has proven a strong correlation with the slit-lamp gonioscopy with a Cohen’s kappa coefficient of 0.65 and an inter-observer agreement of 0.82 in 250 eyes imaged.
The Limitations:
The smartphone camera has evolved rapidly to now house up to 128 megapixels, the sensors though remain woefully small. This prevents us from imaging subtle changes at the angles in the current form. The bright light from the smartphone flash often does not have an option to be dimmed in the camera app, which might lead to a borderline angle-closure suspect to be diagnosed as open-angle. These factors limit the DIGS Pro to be a screening device for classifying the anterior chamber angle rather than a diagnostic device. By closely following up on the development of smartphone cameras, we might sooner than later overcome these limitations.
The Future:
The strength of the device lies in its portability and the in-built storage and high processing capabilities. Coupled with high-speed internet that has now penetrated even into the remote corners of the world, the device is automatically ready to be used in teleconsultation services. With the rear camera of the smartphone being used to transmit the video by an on-field technician, a real-time classification can be performed by a glaucoma expert at the base hospital. In our experience, it takes less than 10 patients to train someone to take a gonioimage using a 4-mirror goniolens. Future development of machine learning and artificial intelligence-based on a library of gonioimages will allow us an on-site classification of the angles by the software itself, and the suspects then can be referred to the hospital for further treatment.
References:
- Keeler MIO [Internet]. MIO [cited 2020 Oct 11];Available from: https://www.keelermio.com/
- iNview® for iPod Touch including iPod Touch [Internet]. Volk Optical [cited 2020 Oct 11];Available from: https://www.volk.com/products/inview-for-ipod-touch-including-ipod-touch
- Miiretcam [Internet]. [cited 2020 Oct 11];Available from: http://miiretcam.com/
- Remidio Fundus On Phone | High Quality Retinal Imaging System [Internet]. [cited 2020 Oct 11];Available from: https://www.remidio.com/fop.php
- Chandrakanth P, Nallamuthu P. Anterior segment photography with intraocular lens. Indian J Ophthalmol 2019;67(10):1690.
- Raju B, Raju NSD, Akkara J, Pathengay A. Do it yourself smartphone fundus camera – DIYretCAM. Indian J Ophthalmol 2016;64(9):663.
- Hertzog LH, Albrecht KG, LaBree L, Lee PP. Glaucoma Care and Conformance with Preferred Practice Patterns. Ophthalmology 1996;103(7):1009–13.
- Sihota R. An Indian perspective on primary angle closure and glaucoma. Indian J Ophthalmol 2011;59(7):76.
- Kumar N, Francesco B, Sharma A. Smartphone-based Gonio-Imaging: A Novel Addition to Glaucoma Screening Tools. Journal of Glaucoma 2019;28(9):e149–50.
- Akkara J, Kuriakose A. How-to guide for smartphone slit-lamp imaging. Kerala J Ophthalmol 2019;31(1):64.
- WHO | Priority eye diseases [Internet]. [cited 2020 Oct 11];Available from: https://www.who.int/blindness/causes/priority/en/index6.html
- Garudadri C, Senthil S, Khanna RC, Sannapaneni K, Rao HBL. Prevalence and Risk Factors for Primary Glaucomas in Adult Urban and Rural Populations in the Andhra Pradesh Eye Disease Study. Ophthalmology 2010;117(7):1352–9.
By,
Dr Nilesh Kumar MBBS, DOMS, DNB,
Innovator, DIGS and DIGS Pro,
Lotus Eye Hospital, Coimbatore,
Madhavi Netralaya, Ara, Bihar,
n.nilesh.kumar@gmail.com