Retinopathy of prematurity (ROP) is a disorder seen in low birth weight and preterm infants affecting posterior segment retinal vessels, that potentially leads to blindness if not screened and treated at appropriate time. It can be mild with no visual defects or it may become aggressive with new vessel formation (neovascularisation) and progress to retinal detachment and blindness. It is one of the emerging leading causes of preventable blindness in infant worldwide.
In India, nearly 7.5 million low birth weight and 3.5 million preterm infants are born every year, among which almost 20% to 52% of this screened neonates are detected with ROP. Seen more in middle-income or low-income countries depending on the level of neonatal and ophthalmology care available and also due to limited health resources.
The major risk factor is very low birth weight, prematurity and high oxygen concentration. Associated risk factors can be sepsis, hemodynamic instability or adverse respiratory or cardiac disease profile.
Preterm infants are not born with ROP and there is a window period of few weeks before sight-threatening features of ROP develops. Intensive neonatal care unit play a very pivotal role to organize timely ROP screening. Even if ROP gets detected at first screening, excellent visual outcome can be achieved in most cases.
With the objective to screen early and prevent blindness, Ministry of Health and Family Welfare, introduced โChild Health Screening and Early Intervention Servicesโ as Rashtriya Bal Swasthya Karyakram-RBSK under National Health Mission. It provides health screening and early intervention services for children, including infants up to six weeks of age.
TELE- ROP
Due to lack of adequate ROP trained ophthalmologist and neonatal unit, it was challenging to reach many rural and remote areas. To overcome this inappropriate ratio, a well synchronised TELE-ROP screening campaign was started. Trained technicians preform examinations on-site, using a portable, wide field, and digital retinal imaging system which are uploaded on a tele โROP software. This images are examined by experts and a further management is planned.

Image 1
We at Aravind Eye hospital, Chennai had started tele-ROP under name of โACT-ROPโ (Aravind Chennai Tele-ROP) to serve the society and reach those people who canโt access us providing them best and affordable treatment so that each newborn can have a good quality of vision and can live an independent life.
Our team consist of trained and accredited level technicians (Zone 1,2,3 level of training), a project manager and a driver (Image 2). Screening is done with a portable paediatric retinal imaging system (FORUS health, 3nethra neo digital wide field imaging) as an alternative to Indirect Ophthalmoscope (Image 3). Retinal images taken by camera can be stored, transmitted to software, reviewed, analysed and sequentially compared over time.

Image 2

Image 3
Our aim is to screen preterm and low birth weight newborns and detect ROP at early stage to prevent blindness.
Which newborns should be screened?
Screening should be carried out for the infants with either of the following:
-Birth weight less than 2000 gm
-Gestational age less than 34 weeks โจ
-Gestational age between 34 to 36 weeks but with risk factors such as: hemodynamic instability or respiratory or cardiac disease profile.
-An unstable clinical course who are at high risk (as determined by the neonatologist or paediatrician). โจ
When to screen?
-Should receive first screening at 4 weeks of birth.
-Infants with birth weight less than 1200grams or period of gestation less than 28 weeks should be first screened at 2-3 weeks after delivery
– Very low birth weight newborns have a tendency to develop early and aggressive form of ROP, such babies should be screened early. Intensive care unit need to be vigilant for such newborns and should ask for early screening.
Frequency of screening?
Follow up examination intervals are based on the retinal findings.
In general, every 1-2 weeks screening is preferred until:
-Vascularization of the retina reaches normal completion- at about 40 weeks of postmenstrual age
-Until ROP regresses
-Until ROP requiring treatment develops
Where to screen?
Ideal place is a neonatal unit with child inside a radiant warmer by a trained ophthalmologist/technician under supervision of attending paediatrician/ neonatologist.
Our trained technicians preform examinations on-site, using a portable, wide field, and digital retinal which are later uploaded on a tele โROP software. This images are examined same day by experts and further plan of action is decided.
Treatment:
Laser therapy is the standard treatment for vision-threatening ROP performed in NICU/SNCU monitored by neonatologist or paediatrician with pulse oximetry monitoring according to the ETROP guidelines. In 2011, the BEAT-ROP prospective study on Avastin (bevacizumab, Genentech/Roche) intravitreal injection brought a new perspective to the treatment of ROP.
Intravitreal injections are reserved mainly for posterior disease where extensive laser close to the macula is needed. Aggressive posterior ROP (APROP) is an emergency situation which does not obey the regular staging, hence requires urgent intravitreal anti vascular endothelial growth factor (VEGF). This may be followed by an eventual laser treatment if vascularisation does not become complete.
Rarely surgery may be required if the stage becomes 4A and 4B. Surgery for stage 5 (closed funnel configuration of retinal detachment) is generally not successful
Universal protocol regarding whom to treat:
Type 1 ROP: Administer peripheral ablation treatment
- Zone I, any stage ROP with plus disease
- Zone I, stage 3 ROP without plus disease
- Zone II, stage 2 or 3 ROP with plus disease

Image 4: Above retina image taken by our wide field imaging system of a preterm infant with Zone 2- Stage 3 with plus disease ROP.
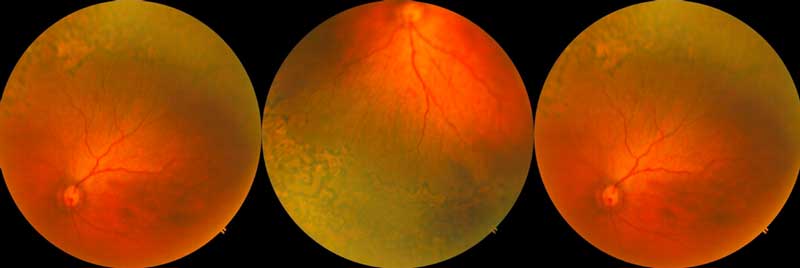
Image 5: Same infant post laser therapy performed by trained ROP specialist.
Type 2 ROP: Wait and watch for progression/regression
- Zone I, stage 1 or 2 ROP without plus disease โ Follow up once a week.
- Zone II, stage 1 or 2 ROP without plus disease โ follow up once in 2 weeks
- Zone II, stage 3 ROP without plus disease- Follow up once a week
Counselling:
Counselling of the parents regarding severity of the disease holds a very crucial step as people living in rural area may not be able to come for follow up.
- Parents of all babies at risk – written general information should be provided with highlighting next date, month of follow up.
- Parents of infants with severe ROP – the ophthalmologist should personally discuss about the disease, availability of treatment, post treatment follow up with the parents.
- Parents of infants with advanced cicatricial ROP and with visual impairmentโIt is important to ensure that children with visual impairment have blind and vocational guidance centres, special schools and organisations for the future support.
Below image shows our trained staff counselling a mother with details given in written pattern.

Image 6: counselling by our trained staff.
In summary, tele-ROP programs provide a useful screening strategy for ROP in semi-urban and rural areas. And we, ophthalmologist at Aravind eye hospital had took a step ahead to screen such babies and prevent blindness due to ROP via our project ACT-ROP.
By,
Dr Prabhu Baskaran,
Aravind Eye Hospital,
Chennai