Management of a Case of Post Traumatic Chronic Cyclodialysis Cleft With Hypotony Using Sewing Machine Technique.
A 38 year old male presented to us with h/o blunt trauma to the eye with shuttle cock 3 months back, BCVA – RE 6/36 n36, LE 6/6 n6, IOP – RE 6 mm of Hg, LE 18 mm of Hg. Anterior segment examination showed RE shallow anterior chamber with clear lens, LE WNL. On posterior segment evaluation vitreous cavity was clear, optic disc margins were blurred all around with minimal elevation, peripapillary retinal oedema, retinal folds and choroidal folds temporal to fovea and peripheral multiple areas of choroidal detachments were noted, LE WNL. OCT was showing multiple choroidal and retinal folds with altered foveal contour with gross optic nerve head oedema, B Scan showed thickened retinochoroidal complex with peripheral choroidal detachment all over. Anterior segment (AS) OCT showed cyclodialysis cleft extending 3-4 clock hours infero – nasaly. Figure 1 (A-E)
Figure Legends
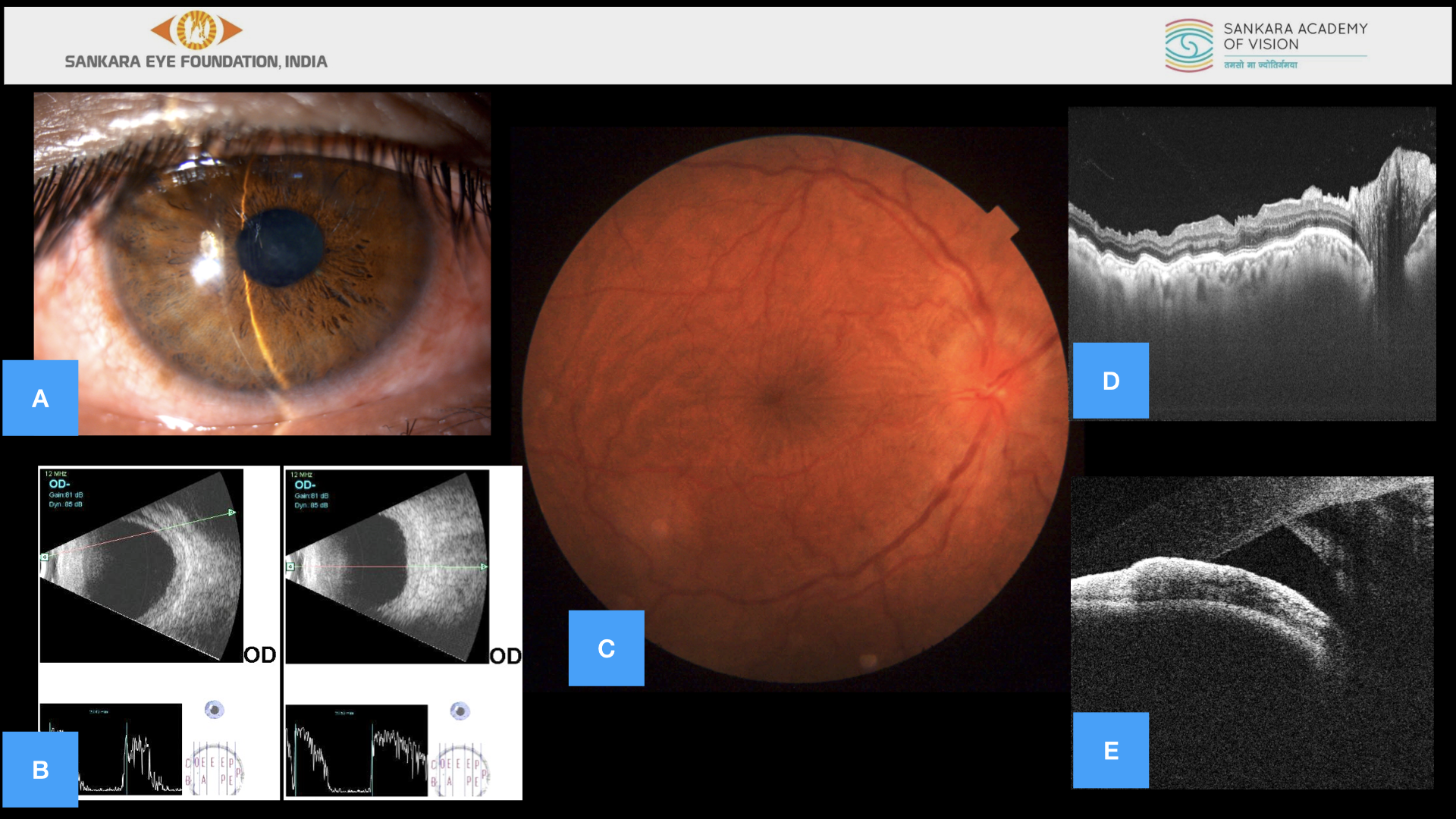
Figure 1 (A-E)
A – Anterior segment photo showing RE shallow anterior chamber with clear lens. B – B Scan showing thickened retinochoroidal complex with peripheral choroidal detachment. C – Fundus photo showing optic disc margins blurred all around with minimal elevation, peripapillary retinal edema, retinal folds and choroidal folds temporal to fovea. D – OCT showing multiple choroidal and retinal folds with altered foveal contour with gross optic nerve head edema. E – Anterior segment (AS) OCT showing cyclodialysis cleft infero – nasaly.
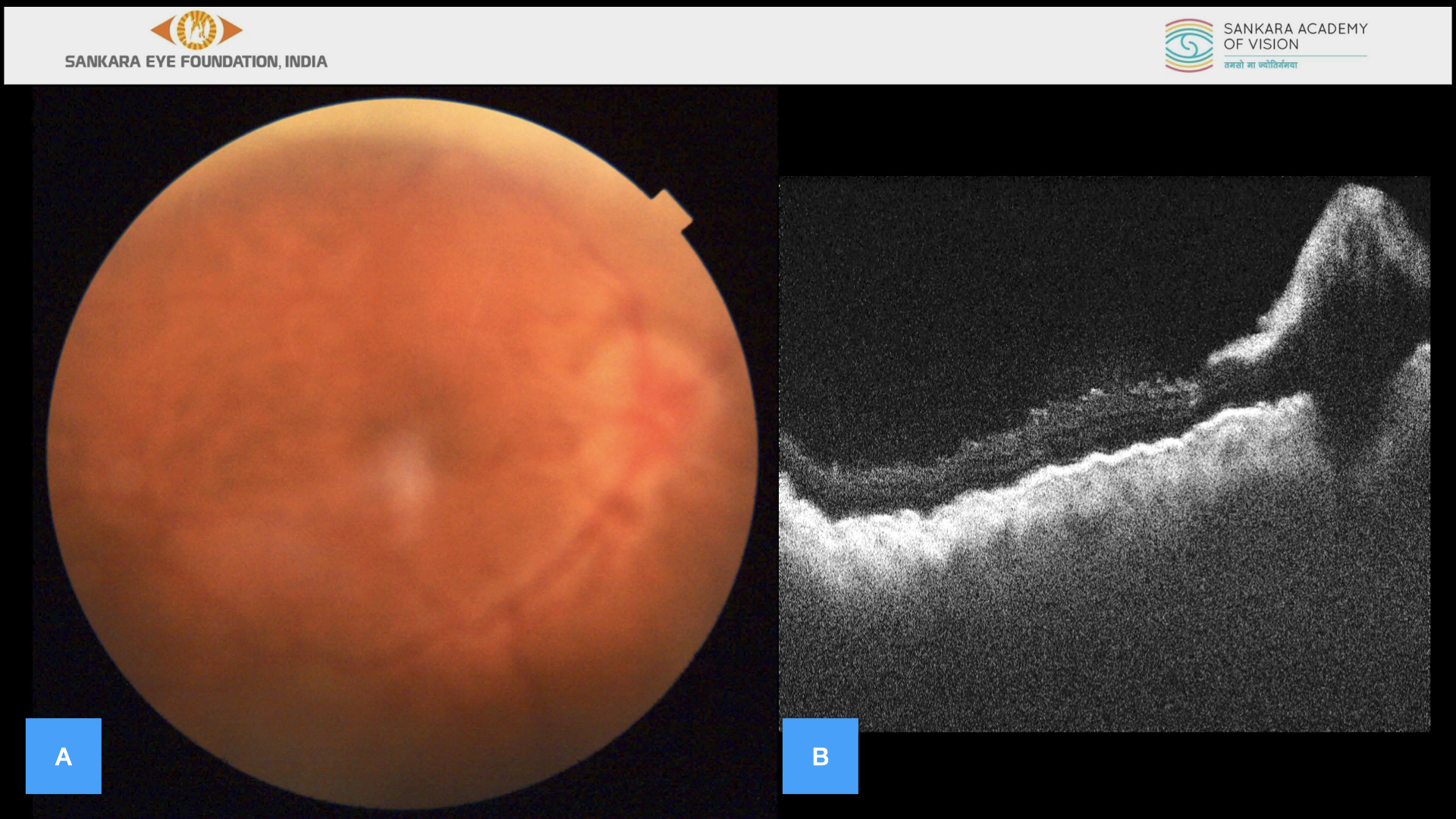
Figure 2 (A-B)
A – Fundus photo showing optic disc margins more blurred with gross elevation, peripapillary retinal edema, retinal folds and choroidal folds also noted to worsen. B – OCT showing grossly worsened multiple choroidal and retinal folds with altered foveal contour with significant increase in optic nerve head edema.

Figure 3 (A-H)
Schematic representation of the important surgical steps – A – The 26G needle threaded with 10–0 Polypropylene suture inserted from the side port. B – The 26G needle threaded with 10–0 suture inserted from the side port engaging the peripheral part of the iris or ciliary body at the site of the cleft in the needle and the needle passed into the site of the scleral groove. C – The 10-0 suture tip emerging from the 26G needle was held with the forceps so as to avoid slipping back. D – Similar manoeuvres performed multiple times to cover the entire extent of the cleft area. E – Each time the 26 needle retracted out of the scleral grove a loop of 10-0 suture is created. F & G – After the last pass of the 26 G needle out of the scleral groove the suture is trimmed to adequate length and exteriorised from the scleral groove. H – Finlay the 10-0 suture was passed from all the loops and tied to the first end forming a single knot.
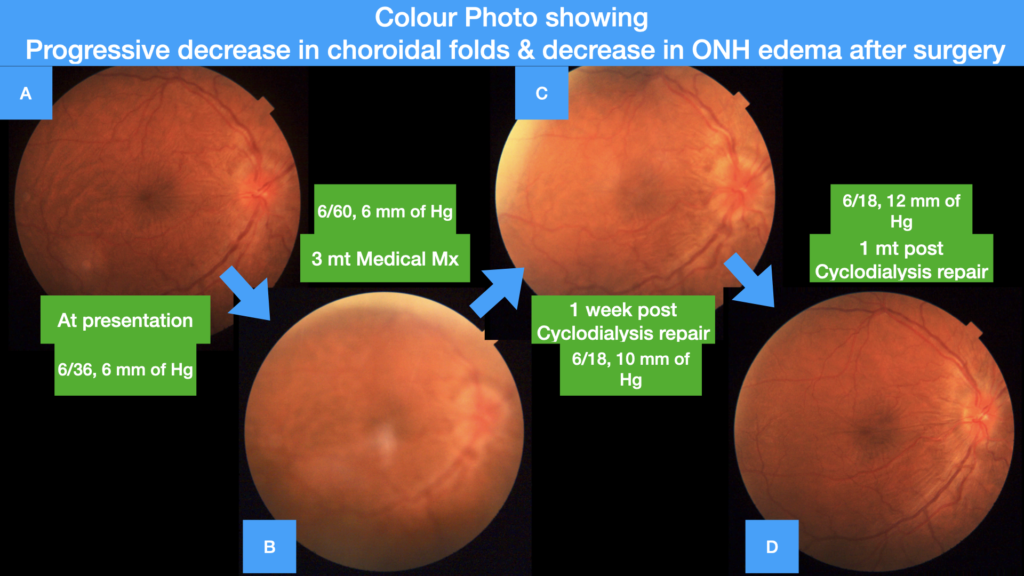
Figure 4 (A-D)
A- Colour Photo at presentation , B- Colour photo at 3 mounds of medical management, C & D – Colour photo post clycodialysis repair surgery showing progressive decrease in choroidal folds and decrease in ONH oedema after surgery at 1 week and 1 month.
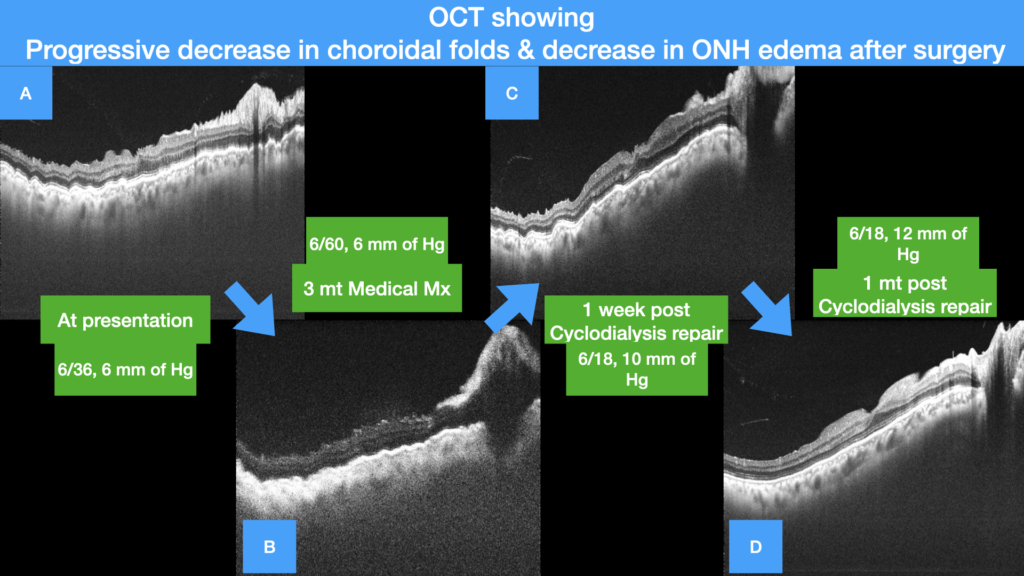
Figure 5 (A-D)
A- OCT at presentation showing multiple choroidal and retinal folds with altered foveal contour with gross optic nerve head oedema, B- OCT at 3 months of medical management showing grossly worsened multiple choroidal and retinal folds with altered foveal contour with significant increase in optic nerve head oedema, C & D – OCT showing progressive decrease of choroidal and retinal folds with restoration of foveal contour with progressive decrease of optic nerve head oedema at 1 week and 1 month.
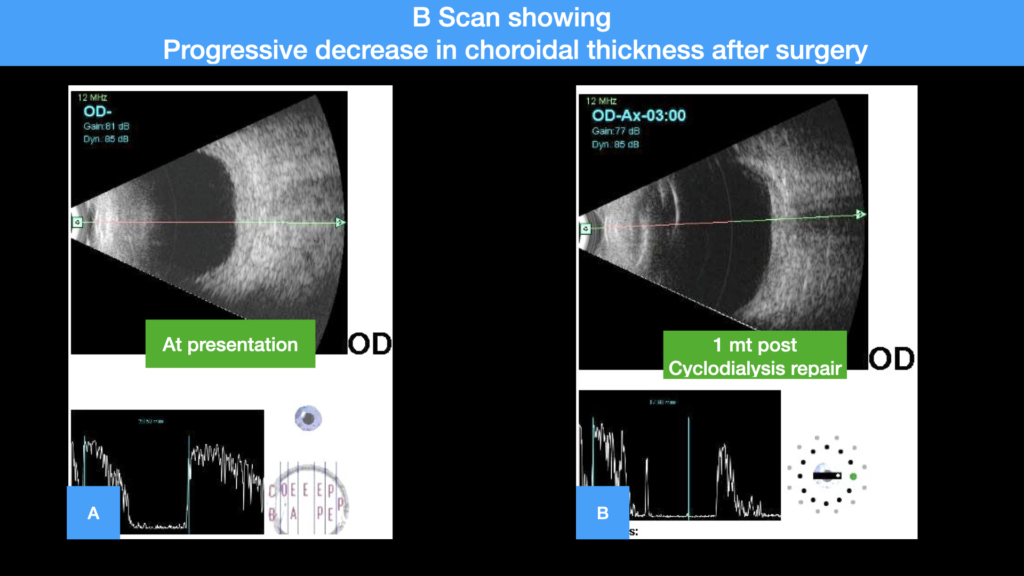
Figure 6 (A-B)
A- B scan at presentation showing grossly thickened retinochoroidal complex, B – B Scan showing decreased thickness of retinochoroidal complex with no choroidal detachment at 1 month post cycodialysis repair surgery.
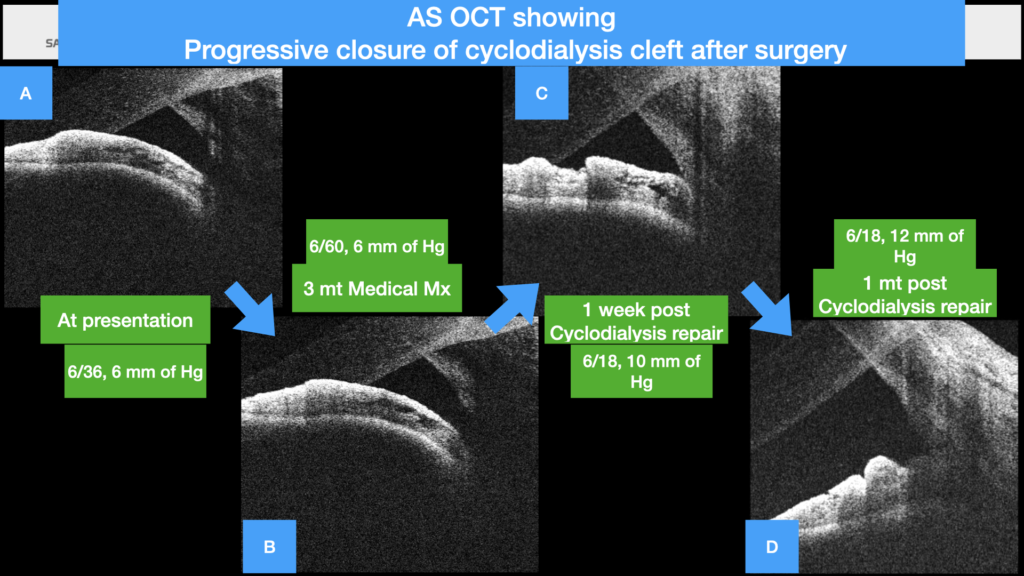
Figure 7 (A-D)
A- ASOCT at presentation showing the cycodialysis cleft , B- ASOCT at 3 mounds of medical management showing the cycodialysis cleft, C & D – ASOCT post clycodialysis repair surgery showing progressive closure of the cycodialysis cleft after surgery at 1 week and 1 month.
Diagnosis of post traumatic chronic ocular hypotony secondary to cyclodialysis cleft was made (3-4 clock hours infero – nasaly) and was started on systemic steroid 1mg/kg, topical hourly steroids & cycloplegics.
The subject lost for follow up and reviewed after 3 months, BCVA – RE 6/36 n36, IOP – RE 4 mm of Hg. Anterior segment examination showed RE shallow anterior chamber with clear lens. On posterior segment evaluation vitreous cavity was clear, optic disc margins looked more blurred with gross elevation, peripapillary retinal oedema, retinal folds and choroidal folds were also noted to worsen and peripheral multiple areas of choroidal detachments were also noted. OCT was showing grossly worsened multiple choroidal and retinal folds with altered foveal contour with significant increase in optic nerve head oedema. Figure 2 (A-B)
He as diagnosed to have of post traumatic recalcitrant cyclodialysis cleft with no response to medical management and was advised cyclodialysis repair. We had proposed the technique of modified ab interno sewing machine endocyclopexy.[1] (Video file)
The surgical procedure is as follows. Direct gonioscopy was performed and the site and extent of the cleft was identified and marked. After limited conjunctiva peritomy was done along the limbus, scleral groove was made 2mm from limbus corresponding to the site of cyclodialysis. The pupil was constricted using intra cameral pilocarpine. Viso elastic was injected into the anterior chamber. The double arm 10-0 Polypropylene suture was threaded into the 26G half inch needle mounted on the 2 cc syringe without the plunger, other needle at the end of the suture was cut to a point that the suture was just seen jutting out of the 26G needle. The needle was bent approximately 45* near the hub for better manipulation. A side port incision was made along the limbus on the opposite side which didn’t give us adequate access to the cleft site, so another side port entry was made at 12 O clock limbus for easy access to the site of the cleft. The 26G needle threaded with 10–0 suture was inserted from the side port and the peripheral part of the iris or ciliary body at the site of the cleft was engaged in the needle and the needle was passed into the site of sclera groove. The 10-0 suture tip emerging from the 26G needle was held with the forceps so as to avoid slipping back. Similar manoeuvres were performed multiple times to cover the entire extent of the cleft area. Each time the 26 needle was retracted out of the scleral grove a loop of 10-0 suture was created. After the last pass of the 26 G needle out of the scleral groove the suture was trimmed to adequate length and exteriorised from the scleral groove. Finlay the distal end of the 10-0 suture was passed from all the loops and tied to the first end forming a single knot. Figure 3 (A-H) (Video file)
Postoperative follow up at 1 months, BCVA RE 6/18 n12, IOP – RE 12 mm of Hg. Anterior segment showing RE normal anterior chamber with clear lens. On posterior segment evaluation RE showed clear vitreous cavity, optic disc margins were noted to be clear and distinct, no peripapillary retinal oedema, retinal folds and choroidal folds were noted and peripheral choroidal detachment had resolved completely, Figure 4 (A-D). OCT of the RE showed no choroidal and retinal folds with restored foveal contour with absence of optic nerve head oedema, Figure 5 (A-D). B Scan showing decreased thickness of retinochoroidal complex with no choroidal detachment, Figure 6 (A-B). Anterior segment (AS) OCT showed no or closed cyclodialysis cleft, Figure 7 (A-D).
Conclusion modified ab interno sewing machine endocyclopexy technique for traumatic cyclodialysis cleft is a safe and effective procedure with little tissue damage and fewer complications.
References
1.Gupta, Shikha & Selvan, Harathy & Gupta, Viney. (2018). Single-suture single-knot ab interno cyclopexy for extensive posttraumatic cyclodialysis: Modified sewing machine technique. Journal of Cataract & Refractive Surgery. 45. 10.1016/j.jcrs.2018.08.031.
By,
Dr Divyansh K Mishra
Consultant Vitreo Retina,
Sankara Eye Hospital,
Bangalore. INDIA
Ph – 8977405171