Kasturi Bhattacharjee MS, DNB, FRCSEd, FRCS (Glasg), Supurna Ghosh MS Sri Sankaradeva Netralaya, Guwahati, Lana Datuashvili MD – European Society of Ophthalmology – SOE YO Committee Member, Georgia.
Introduction(1)
The tear trough is a concave deformity of the orbital fat that is noticeable as a result of inherited anatomical differences and aging. The tear trough is a 2 or 3 cm depression, inferior to the pseudo herniated orbital fat of the lower eyelid. The tear trough deformities can be a challenging area in facial rejuvenation. Treatment options for the tear trough deformities include filler injection, fat grafting, and lower blepharoplasty with fat repositioning or combining fat grafting in the tear trough.
Aim
This article highlights the anatomical nuances of the tear trough and it’s management options. The authors feel there have been ongoing drifts favoring non-surgical approach for management of the tear trough deformity with the help of dermal fillers for filling up the tear trough deformity more accurately and safety as compared to surgery. Proper planning details of the injection approach along with pre and postoperative photographic documentation is the key to a successful procedure and a happy patient.
Keywords
Tear trough anatomy, deformity, dermal fillers, tyndall effect
Background:
The eye is an important window for facial expression, and dermal fillers can gave a large impact on the science of aging and its psychological cognition. Fillers are few of the most prevalent non-surgical interventions for facial cosmoses. Symptoms such as excess sagging skin, droopy eyelids, dark circles as well as wearied looking eyes may be rectifies with dermal fillers. (2)
Material and Methods
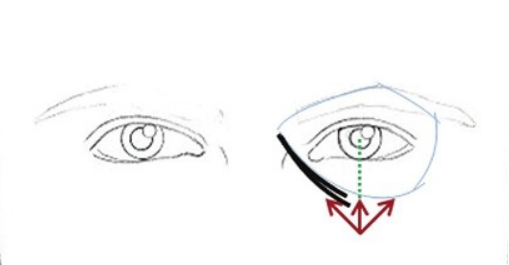
The surgical anatomy of the lower lid is of prime importance (fig.1). The skin of the eyelids comprising of the epidermis and the dermis is the thinnest skin in the body, thereby allowing it for ample stretch during dissection and retraction. It is loosely attached to the underlying muscles rendering it to be a potential site for relatively large quantities of fluid accumulation subcutaneously. Deep to the skin lies the orbicularis oculi muscle (OOM) which is divided into orbital and palpebral portions. The palpebral portion can again be divided into the pretarsal portion (the muscle superficial to the tarsal plates) and the preseptal portion (the muscle superficial to the orbital septum). The bones of the medial orbital rom and the medial canthal tendon give origin to the orbital portion of the orbicularis oculi. Thereafter the peripheral fibers sweep across the eyelid over the orbital margin in a series of concentric loops. In the lower eyelid, the orbital portion merges into the check, after covering the origins of the elevator muscle of the upper lid and nasal ala. The preseptal portion of the orbicularis oculi muscle takes its origin from the medial canthal tendon and lacrimal diaphragm and inserts at the lateral canthus after passing along the lid. The upper and lower pretarsal muscles insert to the common lateral canthal tendon. Medially, the fibers form the medial canthal tendon, inserting form the medial canthal tendon, inserting on the medial orbital margin, the anterior lacrimal crest, and nasal bones. The lower eyelid skin is supplied principally by the infraorbital branch of the maxillary nerve and few branches of the lacrimal and infratrochlear nerves. (3) (4)
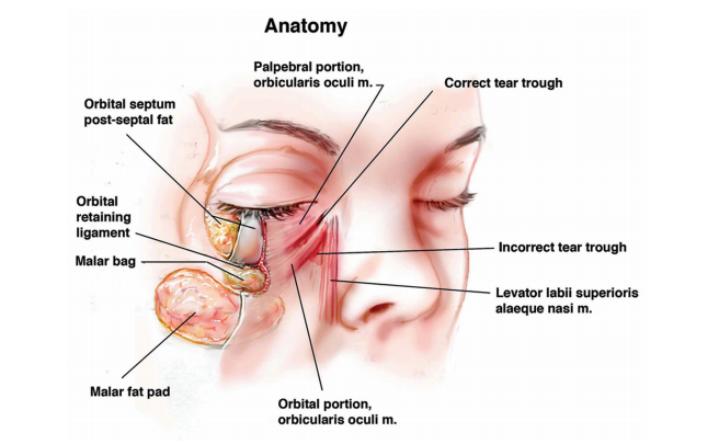
The orbicularis oculi attaches to the inferior orbital rim directly starting from it’s point of origin up to the level of the medial corneoscleral limbus. Thereafter laterally the orbital reataining? ligament forms the indirect attachment between the muscle and the bone. The ligament extends from the orbital rim, to the under surface of the orbicularis. The expanded lateral end of the orbital retaining ligament merge with the lateral orbital thickening (5). This ligamentous expansion has been variously identified as the orbito-malar ligament by Kikkawa et al (6) and the malar septum by Pessa et al (7).
The tear trough ligament has been considered as a true osteo-cutaneous ligament by Wong et al. (8) Goldberg had conceived the idea of the tree hollows: the orbital rim hollow, the zygomatic hollow, and the septal confluence hollow. Of this, the medial portion of the orbital rim hollow is often deepened and corresponds to the tear trough deformity attachment of skin to the bone result in localized hollowing in those regions. Aging on facial region is a function of volume loss. Loss of volume in areas of skin adherent to bone can cause alteration in facial contours which looks like gravitational descent. Identification of these hollows helps in the prototype framework amenable to dermal fillers for rejuvenation. (9) The term nasojugal fold was first introduced by Duke Elder and Wybar in 1961. (10)
Loeb Hypothesized that the “naso-jugal groove“ was due to the anatomical variations: 1) the orbital septum is attached to the inferomedial portion of the arcus marginalis, 2) a triangle shaped deficient area bounded by the angular muscle on one side and the orbicularis oculi muscle on the other. (11)
The term ‘tear trough deformity’ was conceived by Flowers. He postulated that volume loss, descent of aging tissues and poor development of the infraorbital malar complex resulted in the tear trough deformity formation (12).
The location of the tear trough is within the boundaries of the orbicularis oculi muscle. (13)
The term “tear trough deformity” is appropriate for the medial oblique periorbital depression spanning from the medial canthus to the midpupillary line. Lateral to this, the hollowness is the “palpebromalar groove”, “nasojugal groove”, or the “lid-cheeck junction”. (14)
Fig. 2 Barton’s grading system based on anatomic analysis (15)
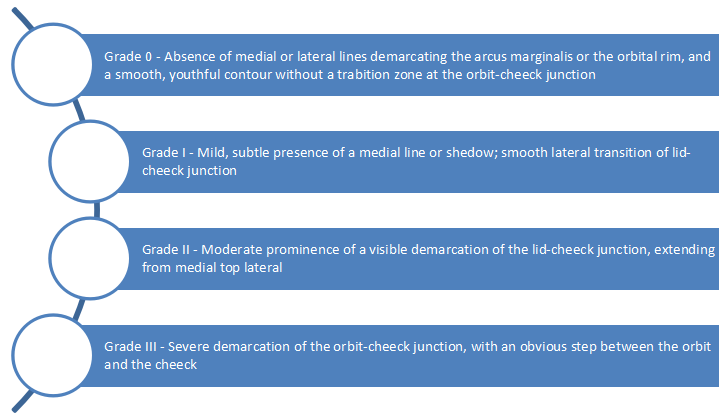
Fig.3 Hirmand’s classification system of the tear trough deformity based on clinical evaluation. (17)
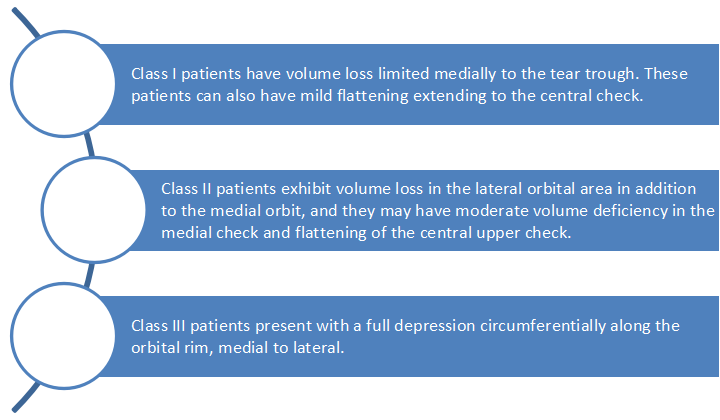
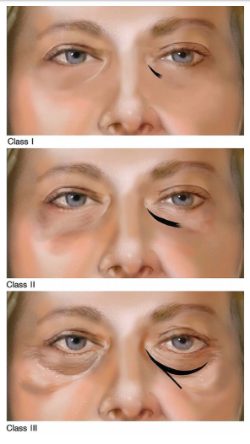
Fig.4 Hirmand Classification of Tear Trough deformity. Adapted from: Hirmand H. Anatomy and nonsurgical correction of the tear trough deformity.
Sidick et el. Developed the TTRS by objectively and subjectively evaluating the clinical appearance of the tear trough with regard to depth of the trough, hyperpigmentation, volume of prolapsed fat and skin rhytidosis.(18)
The New Classification System (19)
Type 1: Hill
Type 2: Valley
Type 3: Hill-Valley
Type 4: Hill-Valley-Hill-Valley
Type 5: Mixed
Evaluation should include a thorough:
- Medical history
- Ophthalmic history including any surgical interventions
- Ocular examination
- Examination of the periorbital skin
- Preexisting dry eye should be assessed and documented preoperatively due to its proportional correlation with postoperative complications.
Physical examination should take into account:
- Lower eyelid position (inferior sclera show and horizontal lid laxity)
- Check projection (tear trough deformity and negative vector calculation) (20)
Assessment of the lower eyelid
Lower eyelid should be assessed for:
- Excess skin tissue
- Fat herniation, which may be medial, central and lateral fat pads. Lower eyelid fat becomes more prominent in upgaze and less prominent in downgaze distinguishing it from periorbital edema
- Slackening of the lateral canthus (due to disinsertion or laxity of the lateral canthal tendon. Snap test or snap back test can assess the degree of laxity and the amount of canthal repositioning required.)
- The orbital rim hypoplasia in relation to the anterior cornea and lower lid margin, a negative vector, should be examined preoperatively.
- Exophthalmos or enophthalmos must be documented with exophthalmometry.
Photographic documentation of pre and post procedure condition after proper written informed consent is advisable. Even navigation guided assessment of the tear trough deformity may be undertaken which helps in better correction and producing symmetrical results on the two sides. The expectations and concerns of the patients undergoing a cosmetic procedure must be accounted for, and the pros and cons be well explained while counselling the patients. The use of a hand mirror to demonstrate the desired changes is always a welcome step and goes a long way in relieving patient concerns.
Blepharoplasty has been the traditional approaches to e tear trough deformity for obtain a smooth lid check junction. Vascularized fat pedicle to fill up the tear trough was propagated by Hamra by modifying Loeb’s fat sliding technique. (21)
Microfat grafting is a great alternative for augmentation of patient with post blepharoplasty hollowing specially after classical fat sculpting techniques. (22)
Aspiration and re-injection (liposculpture) of autogenous fat though small incisions providing excellent results. (23)
The recent use of autologous fat injection or hyaluronic fillers to replace periorbital volume has saved the day for cases not amenable to traditional blepharoplasty due to soft tissue atrophy. (24)
Dermal Fillers
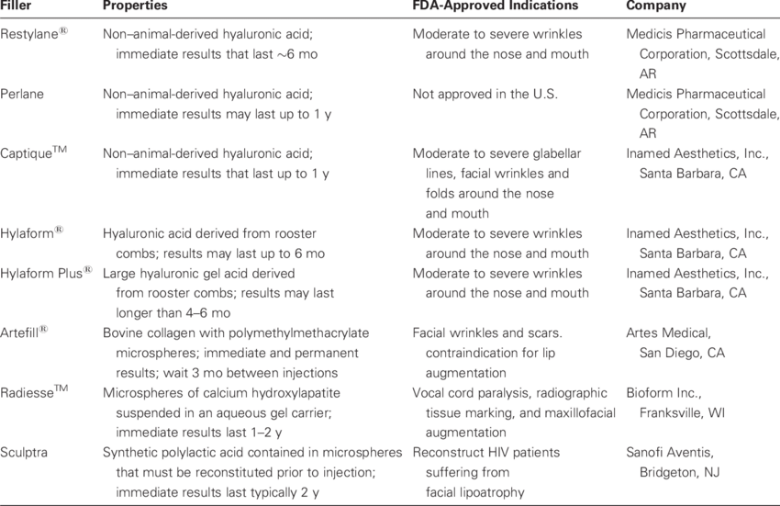
Fillers are substances used for augmentation of soft tissues of fill up the volume attrition due to subcutaneous fat loss associated with aging. (25) With increasing age, the body’s natural potential to produce hyaluronic acid as well as its inherent hygroscopy decreases thereby playing an important role in facial soft tissue atrophy. Fillers are primarily indicated for volume augmentation and correction of static rhytides. They restore symmetry and the volume loss on the face. Soft tissue fillers help in re-augmentation of the depleting collagen. Main modality of its action is to impregenate the soft tissue and or peritoneum to support and lift the fat pads and ligaments. The role of dermal fillers for facial aesthetics has revolutionized with the introduction of Hyaluronic acid (HA) fillers. The newer Hyaluronic Acid (HA) based agents has restored the interest in dermal fillers as they promise better outcomes with a lesser side effect. The first HA filler approved by FDA was Restylane in 2003. Since then, HA fillers have been the crux for volume augmentation and facial rejuvenation.
Classification (26)
Fillers can be classified depending on the duration of effect, material of origin, and reversibility. Depending on duration of effect they may be classified as short (less than 3 months), medium (3-12 months), long (12-24 months), or very long acting (more than 24 months).
HA soft tissue fillers are manufactured using two different of technologies:
Earlier fillers based on Hylacross, which utilizes crosslinked high-molecular weight HA were in use. Recently VYCROSS technology utilizes an innovation combination of low and high molecular weight HA which enhances the cross-linking efficiency of HA chains. (27)
Benefits of VycrossTM Technology:
- The filler is much smoother with a natural look
- Easier to inject, therefore less pain when injecting
- Difficult to perceive any filler in skin
- Result usually persist up to 18 months.
Hyaluronic Acid Derivatives (HA)
Hyaluronic acid is a non-animal, non-cadaver polysaccharide biomolecule, naturally occurring compound, which forms a part of the normal extracellular matrix of the dermis and connective tissue. (28) Thus they are biocompatible with no immunogenicity. It has a set of properties, which makes it a desirable agent for injection. Its hydrophilic property and the ability to imbibe water, makes it natural filler.
It is rapidly degraded is its natural form and needs to be cross-linked for stabilisation. Various commercial preparations of HA differ on the basis of the following aspects: the source, concentration, particular size, cross-linking, type of crosslinking agents being used, and whether the HA is monophasic (more cohesive & do not migrate) or biphasic (customized for particular anatomic area), and whether an anesthetic has been added. The injection technique as well as the filler type should be customized to which area is to be treated. It is always better to undertreat, as HA fillers will expand as they imbibe water overnight.
Adverse effect include pain, bruising, edema, nodule formation, accidental intravascular injection, Tyndall effect (if the injection is given too superficially and the skin is very thin), granuloma, scarring, even blindness resulting from central retinal artery occlusion.
Technique
Preoperative consent is a must and like any cosmetic procedure, the patient is given mirror and asked to pint out the areas where he/she feels require treatment, 1% Lignocaine topical cream (Prilox, Elma, etc) is applied 30-40 minutes 30 minutes prior to the filler injection. Cold compress and inferior alveolar nerve block have also been used for anesthesia. (29) The desired areas are then cleaned with isopropyl alcohol or chlorhexidine. Rich subdermal vascular plexus, predispose the tear trough area to significant bruising, the point of insertion of the needle about 1.5 cm below the orbital rim in line with the midpupillary line causes significant reduction in bruising (fig.3). Superficial injection tends to give a Tyndall effect in this area. Another depot injection is given in the subperiosteal plane in the mid pupillary line. Thereafter the direction of the needle is directed towards the lateral canthus and subperiosteal injection given. Usually about 0.2 ml per site advocated. Gentle massage enables product distribution and to rule out lumps and bumps.
Care is taken to inject away from any visible blood vessels in this area. Ice packs help to reduce edema, bruising and discomfort. (30, 31)
The use of blunt cannulas for dermal fillers started back in 2011. The incidence of bruising and Tyndall effect was found to be significantly lesser when injected with blunt tipped cannula. The length of the cannula being longer the access to the extreme medial end of the tear trough was possible with a single point of insertion.
The authors has shifted to the use of blunt tipped cannula and have found better results immediately post procedure as well as long term outcome were way much satisfactory.
Posttreatment Management:
1. The patients should avoid strong or extended pressure within the treated area.
2. The patients should be informed about after care such as avoiding massage, strenuous physical activity and exposure to extreme cold or heat for up to six hours post treatment.
3. It is important to schedule follow up sessions to assess the clinical result. Touch ups may be performed in the follow up sessions if required
Conclusion
Soft tissue fillers offer an excellent non-surgical method of managing the Tear trough defect with effacement of Lid Cheek Junction. A thorough knowledge about facial anatomy is an important because before attempting to inject them.
References:
- Jindou Jiang1 , Xuekun Wang2 , Rongrong Chen1 , Xueying Xia1 , Sai Sun1 , Kuikui Hu1 – Tear trough deformity: different types of anatomy and treatment options
- Glaser DA, Patel U. Enhancing the eye: Use of minimally invasive technique for periorbital rejuvenation. J Duds Dearmatol. 2010˜9:118-283
- Casto E. Foster JA. Upper lid blepharoplasty. Facial Plast Surg. 1999; 15(3):173-81.
- Hwang K, Lee DK, Lee EJ, Chung IH, Lee Sl. Innervation of the lower eyelid in relation to blepharoplasty and midface lift: clinical observervation and cadaver study. AnnPlast Srg. 2001 Jul; 47(1):1-5
- Hwang K, Nam YS, Choi HG, Han SH, Hwang SH, Cutaneous innervation of lower eyelid. JCraniofac Surg. 2008 Nov; 19(6):1675-7
- Muzaffar A R, Mendelson B, Adams W, Surgical Anatomy of the Ligamentous Attachment of the Lower Lid and Lateral Canthus, Plastic And Reconstructive Surgery, Sept 2002
- Kikkawa, D. O, Lemke, B.N., and Dortzbach, R.K. Relationsof the superficial musculoaponeurotic system to the orbit and characterization of the orbitomalar ligament. Ophth. Reconstr. Surg. 12:77,1996
- Pessa, J.E., Zadoo, V.P., Adrian, E.K., et al. Anatomy of a “black eye”: A newly described facial system of the lower eyelid. Clin. Anat. 11:157,1998.
- Wong CH. The tear trough ligament: anatomical basis for the tear trough deformity, PlastReconstrSurg. 2012 Jun;129(6):1392-402
- Goldberg Robert A, The Three Periorbital Hollows: A Paradigm for periorbital Rejuvenation: Nov2005;116(6):1796-1804
- DukeElder S, Wybar KC. The eyelids. In: DukeElder S, editor. System of Ophthalmology: Anatomy of the visual system. Vol. 2. St Louis, MO: C V Mosby CO˜1961
- Loeb R. Nasojugal groove leveling with fat tissue. ClinPlastSurg. 1993˜20:393-400
- Flowers RS. Tear trough implants for correction of tear trough deformity. ClinPlast Surg. 1993˜20:403-15
- Haddock NT, Saadeh PB, Boutros S, Thorne CH. Thetear trough and lid/check junction: anatomy and implications for surgical correction. Plast Reconstr Surg. A. 2009;123(4):1332-1340
- Muzaffar AR, Mendelson BC, Adams WP. Surgical anatomy of the ligamentous attachment of the lower lid and lateral canthus. PlastReconstrSurg 2002;110(3):873-884.
- Barton EE. Jr, Ha R, Awada M. Fat extrusion and septal reset in patients with the tear trough triad: A critical appraisal. PlastReconstr Surg. 2004˜113:2115-2
- Peng PH. Treating the tear trtough: A new classification system, a 6-step evaluation procedure, hyaluronic and injection algorithm, and treatment sequences
- Hirmand H. Anatomy and nonsurgical correction of the tear trough deformity. PlastReconstr Surg. 2010˜125:699-708
- Sadick NS, Bosniak SL, CantisanoZ, M, Glavas IP, Roy D. Definition of the tear trough and the tear trough rating scale. J CosmetDermatol. 2007˜6:218-22
- Turkmani M, New Classification System for Tear Trough Deformity; DermatolSurg 2007;0:1-5
- Naik M, Honavar S, Das S, Blepharoplasty: An Overview. J CutanAesthet Surg. 2009 Jan-Jun; 2(1):6-11
- Loeb R. Fat pad sliding and fat grafting for leveling lid depression.ClinPlast Surg. 1981 Oct. 8(4):757-76
- Tonnard P, Verpaele AM, Zeltzer AA. Augmentation blepharoplasty: a review of 500 consecutive patients. AesthetSurg J. 33(3):341-52
- Silkiss R Z, Baylis H I. Atogenous fat grafting by injection. Ophthal Plast Reconstr Surg. 1987˜3:71-75
- Tonnard P, Verpaele AM, Zeltzer AA. Augmentation blepharoplasty: a review of 500 consecutive patients. AesthetSurg L. 2013 Mar. 33(3):341-52
- VedamurthyM. Standart guidelines for the use of dermal fillers. Indian J Der, atolVenerolLeprol 2008;74, Suppl S1:23-7
- Smith KC. Reversible vs. nonreversible fillers in facial in facial aesthetics: concerns and consideration. Dermatol Online J 2008;14(8):3
- Dormston W, Hilton S.A prospective, open label, multicenter, observational, postmarket study of the use of 15mg/ml hyaluronic acid dermal fillers in lips. J Cosmet Dermtol. 2014 Jun; 13(2):125-134
- Jordan DR. Soft-tissue ullers for wrinkles, folds and volume augmentation. Can J Ophthalmol. 2003;38(4):285-8
- Beasley KL, Weiss MA, Weiss RA. Hyaluronic acid fillers: a comprehensive review. Facial Plast Surg. 2009;38(4):285-8
- Dermal Fillers For the treatment of Tear Trough Deformity: A Review of Anatomy, Treatment Techniques, and their Outcomes Jaishree Sharad J CutanAesthet Surg. 2012 OctDec˜5(4):229-238.
- Bray D, Hopkins C, Roberts DN. A review of dermal fillers in facial plastic surgery. CurrOpinOtolaryngol Head Neck Surg. 2010;18(4):295-302