Fundoscopy is known for years as a diagnostic and therapeutic window to study systemic hypertension (HTN). The extent of end-organ damage secondary to it can be studied by direct observation of arteriolar changes in the fundus. Earlier, these findings were the crucial deciding factors to intervene and manage the ill effects of HTN.
Of late in the management of HTN, the dependency on fundus findings has gone to the corner with the evolution of better biomarkers to assess end-organ damage. Currently, ophthalmologists focus mainly on complications related to it viz optic neuropathies, retinal arteriolar & vein occlusions, and choroidopathy. Mere retinal changes like focal ischemic changes are largely ignored if underlying systemic HTN is under control. Hypertension is less common in young people, these findings are often overlooked or misdiagnosed if neither the ophthalmologist nor the subject is aware of the undiagnosed underlying HTN.
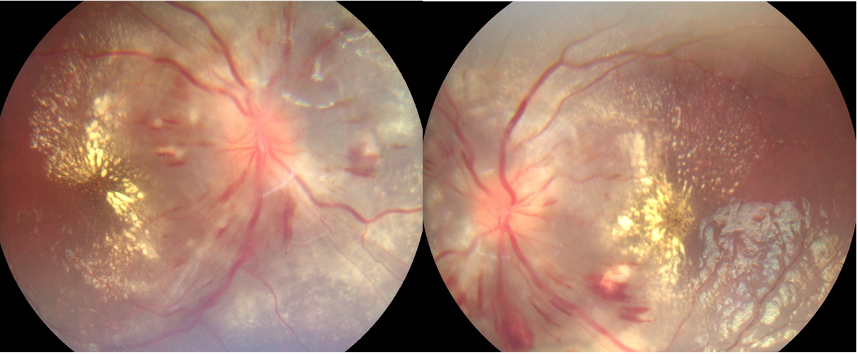
In young, severe HTN causes arteriolar narrowing resulting in ischemia of nerve fiber layers seen as cotton wool spots and vascular endothelial injury noted as a blot and flame hemorrhages. Transudation results in macular and disc edema (in very severe cases) and in the long-run lipids precipitate, forming varying extent of the macular star. (Figure) In extensive cases, ischemia of the choroidal vascular layers causes exudation of fluid under the retina causing retinal detachment and chronic changes leading to atrophy of overlying RPE.
The retinal changes described above mimic commonly occurring uveitic diseases in young viz neuroretinitis, papillitis, autoimmune and collagen vascular disorders. The worst scenario can be exacerbating the systemic HTN with intense, prolonged steroid therapy with the overenthusiasm of controlling a misdiagnosed uveitic entity. The suspicion of HTN-R is not borne if history doesn’t reveal systemic disease or subjects are asymptomatic except for eye changes. Leibriech et al described albuminuric retinitis for retinal changes in the young who are hypertensives secondary to underlying kidney diseases. Of late, similar findings are seen more in young with primary HTN.
Despite being a common disease, HTN is considered a disease of the elderly. Many adolescents and younger individuals under the age of 30 are left from the ambit of screening for HTN. A low threshold to screen for high blood pressure when retinal changes are observed not only uncovers the hidden systemic HTN but also avoids unnecessary investigations. The optic atrophy and macular thinning due to chronic ischemia are irreversible and can be visually disabling. Arriving at the right diagnosis by the ophthalmologist can be rewarding, not only for his clinical acumen but also for the right intervention which when taken by the physician/ pediatrician can often be life-saving.
Authors
Dr. Steffi Rose Prasad,
Dr. Nagesha C K. (MS, FMRF)
contact mail : drnageshck_2006@yahoo.com
B W Lions Superspeciality Eye Hospital
Bangalore, Karnataka
INDIA