Dr Swati Singh, Dr Bharat Ratna Thoumungkan, Dr Surbi Taneja, Centre for Sight, Safdarjung Enclave, New Delhi
Introduction
Uveitis affects 2 million people worldwide out of which about 10% may suffer from irreversible loss of sight due to associated complications.1,2 Cystoid macular edema, cataract and glaucoma are the three major causes of visual loss in patients with uveitis.3 Glaucoma is ranked as the third most common complication in uveitis after cystoid macula edema (CME) and cataract.4
Cataract formation and glaucoma in patients with uveitis is usually caused by chronic inflammation along with prolonged use of high-dose topical, periocular and/or systemic corticosteroids.5 Chronic anterior uveitis is known to cause irido-lenticular synechiae formation which obstruct the normal aqueous humour circulation from posterior to anterior chamber. Annular or ring synechiae between pupillary margin and lens lead to gradual iris bombe’ formation with peripheral shallow AC depth and secondary angle closure glaucoma.6
Chronic uveitis may also lead to formation of fibrinous membrane in pupillary area causing a uniformally shallow or flat anterior chamber which may be falsely interpreted as malignant glaucoma. Intraocular pressure may be extremely high in such eyes making the patient highly symptomatic. An urgent intervention is needed to reduce pain and prevent corneal decompensation as well as to save potential vision in seeing eyes.
Case Report
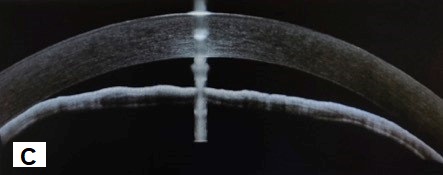
A 64-year- old man who was a known case of Diabetes mellitus, coronary artery disease presented with severe pain and redness in left eye for a fortnight. He gave a history of head trauma in childhood followed by recurrent uveitis and diminished vision in left eye for more than 20 years. He was using eye drops dorzolamide, brimonidine with timolol combination and homatropine in left eye. Last attack of uveitis had happened 8 years ago and since then there were no symptoms till this recent episode. On examination, his right eye anterior and posterior segments were within normal limits. Left eye examination showed a vision of Perception of light with inaccurate PR. Intraocular pressure (GAT) was 48 mm Hg. Slit lamp examination revealed circumcorneal congestion with Corneal haze. Anterior chamber (Fig A) was obliterated in periphery and extremely shallow in centre. However, there were no signs of flare up of uveitis. Pupil was pinpoint with a fibrous membrane bridging the pupillary area completely (Fig B). Anterior segment OCT confirmed the clinical anterior segment findings (Fig C).
B-scan USG showed lens echoes and vitreous degeneration. Retina- choroid complex was within normal limits.


Management
Patient was advised administered topical steroids along with systemic and topical antiglaucoma medication. Nd: YAG laser was used to perforate the tough fibrous tissue causing occlusion pupillae using low energy (0.7-0.8 mJ) in anterior offset setting (Fig D). Perforation of membrane immediately deepened the chamber causing the iris to fall back (Fig E). Small hyphaema was formed by bleeding from pupillary margin which cleared in a week (Fig D). Repeat OCT showed high peripheral anterior synechiae creating a pseudoangle (Fig F) and deepened AC (Fig G). IOP post laser on maximum medication was 32 mmHg.




Two weeks later, Phacotrabeculectomy with MMC with synechialysis was done under steroid cover using iris hooks under intravenous injection Mannitol under local peribulbar anaesthesia (Figures H-I). The hard, leathery cataract was successfully removed and a single piece IOL was implanted in the bag and peripheral synechiae were released with a manipulator. A diffuse bleb was seen on day 1 (Fig J). One-month later, IOP was10 mm with a well-formed AC. Patient regained a vision of FC at 1 metre and Fundus examination showed glaucomatous optic atrophy with disc pallor. 3 months post-surgery patient was stable with IOP 26 mm Hg and Timolol 0.5 % drop was added at this time in left eye.



Discussion
This case is interesting as it showcases two different mechanisms of glaucoma in a uveitis patient caused by occlusio pupillae and secondary angle closure. Lack of keratic precipitates and AC cells ruled out a flare up of uveitis. As the central anterior chamber was not completely obliterated, a laser procedure could be done which was successful in providing immediate relief by reducing IOP and pain. However, as the angles were already closed by PAS formation due to prolonged peripheral irido -corneal contact, a second surgery was required to control IOP. We faced a management dilemma at this time as to whether to do a cyclodestructive procedure or a combined cataract and glaucoma surgery. But as the post laser assessment showed a leathery hard cataract, we planned to remove the huge cataractous lens and create space in the eye along with an augmented trabeculectomy under explained highly guarded visual prognosis.
Conclusion
Management of uveitic cataract with refractory secondary glaucoma is extremely demanding with high risk of complications and failure of filtration procedure. Even if the patient has a slightest chance of recovery of vision, meticulous treatment plan needs to be implemented. Laser procedure to cut the fibrous tissue in pupillary area can help in AC reformation and reducing the uncontrollable intraocular pressure as well as in deciding the further course of action.7
References:
- Siddique SS, Suelves AM, Baheti U et al. Glaucoma and uveitis. Surv Ophthalmol. 2013;;58::1-–10.
- Neri P, Azuara-Blanco A, Forrester J.V, 2004. Incidence of glaucoma in patients withuveitis. J. Glaucoma 13 (6), 461–465
- Durrani OM, Tehrani NN, Marr JE, Moradi P, Stavrou P, Murray PI, et al. Degree, duration, and causes of visual loss in uveitis. Br J Ophthalmol. 2004;88:1159–62.
- Heinz C, Koch JM, Zurek-Imhoff B, Heiligenhaus A. Prevalence of uveitic secondary glaucoma and success of nonsurgical treatment in adults and children in a tertiary referral center. Ocul Immunol Inflamm 2009;17:243-8.
- Kalogeropoulos D, Sung VC. Pathogenesis of Uveitic Glaucoma. J Curr Glaucoma Pract. 2018 Sep-Dec;12(3):125-138. doi: 10.5005/jp-journals-10028-1257.
- Rumelt, S. . Uveitic Glaucoma. In: Rumelt, S. , editor. Glaucoma – Basic and Clinical Aspects [Internet]. London: IntechOpen; 2013
- Kumar H, Ahuja S, Garg SP. Neodymium: YAG laser iridolenticular synechiolysis in uveitis. Ophthalmic Surg 1994;25:288-91.